Thesis, evidence, and buyer actions
Frames the domain, strategic thesis, opportunities, risks, limitations, near-discovery signals, and what different buyers should do next.
Each Zemi dossier pairs a ~100-page decision report with its real engine: a 30-to-45-sheet Evidence & Decision Workbook you operate — a live power-calculation engine, an executable classifier, a full source-audit trail, and 13+ falsifiable, pre-powered hypotheses — built from hundreds of verified sources.
The complete PDF research report and the Evidence & Decision Workbook with live, editable power calculations. Single-license, secure Stripe checkout.
Describe your indication, target, or diligence question and we'll point you to the right dossier — or scope a custom one in a domain we haven't published yet.
See a single dossier hypothesis carried all the way to a full clinical trial design — the worked fibrosis example, published in full.
The report makes the argument; the workbook is where the value lives — an auditable evidence system plus two working tools, in one spreadsheet you drive with your own numbers. It is included with every dossier, and it is the most valuable thing in the package.
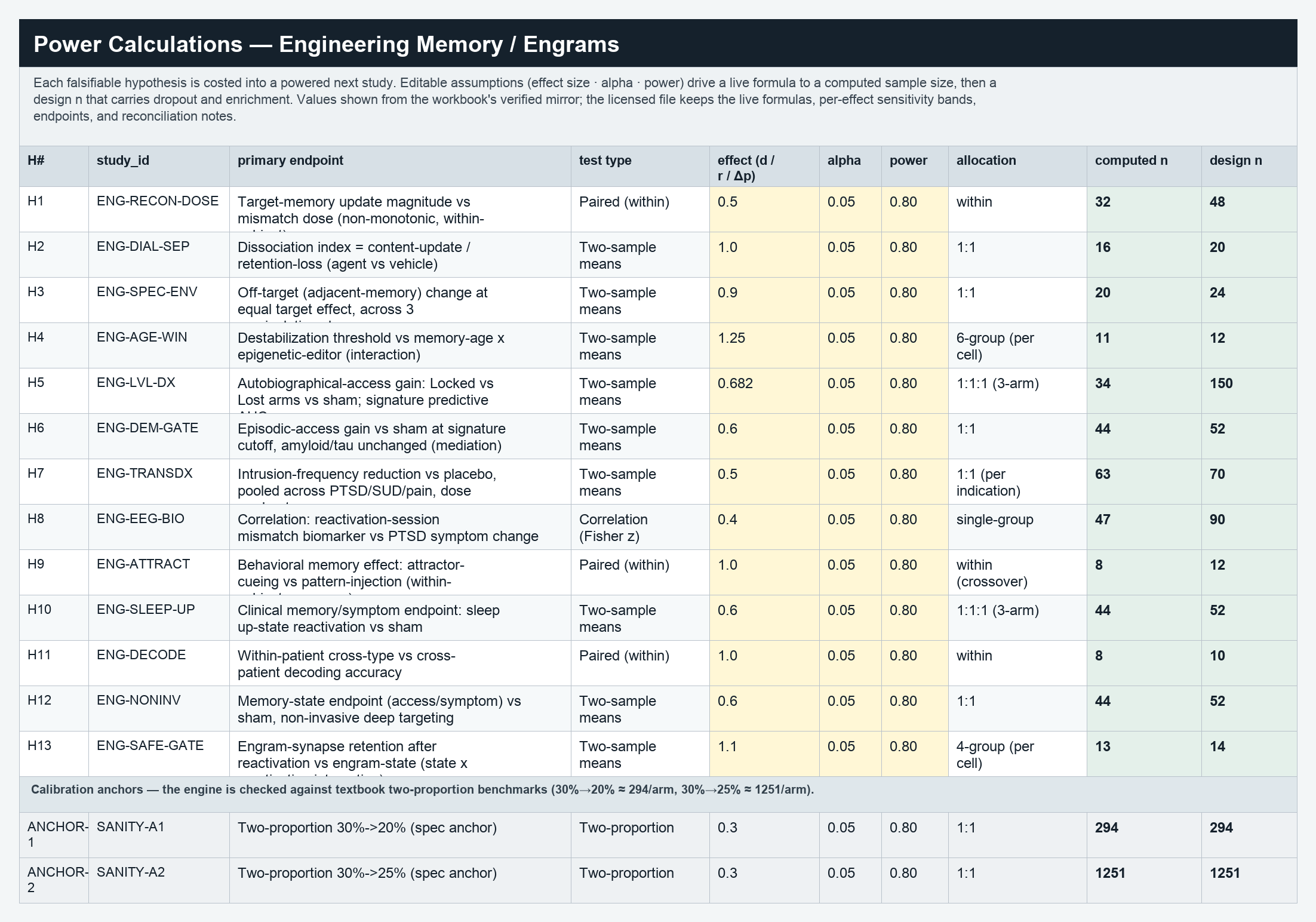
Every hypothesis rendered as live NORM.S.INV sample-size formulas with per-effect sensitivity bands and a cached-vs-live integrity check. Change the effect, control rate, or alpha and every required n recomputes — model your own program in the first meeting.
Enter your program's profile and it returns the binding (rate-limiting) node, the matched strategy, the required assay panel, and a safety-critical contraindication — with its own decision rules, organ rules, archetype cards, validation log, and traceability map.
Claim Ledger, Evidence Table, Source-Support Verdicts (supports exactly / partially / contradicts / insufficient), Source-Quality Summary, and a Traceability Certificate — each claim carrying a verbatim excerpt and identifier, retraction-checked.
A Hypotheses Ledger and a Most-Valuable-Next-Studies sheet: each hypothesis couples ≥2 mechanisms, predicts a readout, names its explicit disconfirming test, and pairs with a costed, powered next study.
Asset & company tracker, trial-catalyst tracker, competitive landscape, regulatory-endpoint tracker, organ-strategy and cross-transfer matrices, and biomarker maps — the moving pieces of the field, sourced and current.
Excluded-claims and quarantined-source registers, a salvage ledger, a full verification & search log, a figure source map, a version registry, and an audit issues log — the discarded and contested material kept in the open.
These are not generic literature reviews, market summaries, or automated article bundles. They are premium medical research-intelligence products designed to help serious builders and funders decide where frontier medical research is actually investable, testable, strategically defensible, or too early.
Frames the domain, strategic thesis, opportunities, risks, limitations, near-discovery signals, and what different buyers should do next.
Shows claim ledgers, evidence tables, source-support verdicts, excluded claims, score basis, traceability certificate, and audit surfaces.
Converts conclusions into explicit, evidence-linked hypotheses, each with a primary endpoint and threshold, the named result that would falsify it, and the validation gates that would strengthen, weaken, or break the thesis. Near-discovery propositions, not proven claims.
Pairs each major hypothesis with population, intervention, comparator, and endpoint, then effect-size, alpha, target power, computed sample size, design sample size, budget, and timeline — and the buyer decision each study resolves.
This preview shows how the Dossier format moves from evidence narrative to inspectable decision infrastructure: report preview, workbook power sheet, traceability surfaces, hypotheses, and limitations.






























The slow, expensive, easy-to-get-wrong part of frontier research is the synthesis: reconciling hundreds of sources into a base of deep, non-obvious connections and falsifiable hypotheses no single reader could assemble. Once you own that base, you can carry a hypothesis past the literature into genuinely new findings. We prove it on our own dossiers — we took a hypothesis beyond the synthesis, pre-registered the analysis, ran it in open reproducible code, and published new frontier results. That advantage is what a dossier hands you.
Starting from the dossier's synthesized base, we pushed its two-population hypothesis into new public-data analysis — four cohorts, 312,929 single cells — and found that matrix formation is molecularly decoupled from lung function and run by a different cell population than degradation. A genuinely new result that pinpoints the patients today's trials can't see. Published, pre-registered, reproducible.
From the dossier's rejuvenation-transformation margin framework, we ran a new pre-registered cross-organ analysis and showed the PRC2 methylation "clock" is proliferation-linked (ρ = +0.85) — a novel result that sharpens the field's core rule (price the margin, not the clock) and opens a fresh question about where the reversible signal really lives. Frontier work the dossier's base made possible.
The synthesized base is what lets a team take one hypothesis — using only public data and simulation, no wet lab — to a trial-design-grade, pre-IND-ready design. To show what's possible, we did it on the fibrosis dossier and published the full trial design.
Replace assumptions with evidence — the number that decides everything.
A biomarker-enrichment design from our own pre-registered analysis.
The true probability of success — a defensible number for an investment committee.
A 20,000-replication adaptive trial that stops early and cheaply when the effect isn't there.
The exact FDA qualification path that makes the trial legal in the first place.
We carried the fibrosis dossier's Hypothesis 1 to a full clinical trial design — 22 linked analyses across ~19 disciplines. A single fixed trial was an honest 57% coin-flip, so we designed an adaptive trial that holds type-I at 2%, gives 82% power, and cuts enrollment from 160 to ~101 patients when the drug doesn't work.
See the fibrosis clinical trial designIt does not run the trial, prove the biology, or replace toxicology. The efficacy effect is trial-measured. That honesty is the brand.
This is the section the top Dossiers tab now lands on: the nine corrected domains, their primary Zemi Dossiers, and the package stats buyers need before choosing a dossier or domain page.
Cancer biology, molecular residual disease, recurrence prevention, immuno-oncology, therapeutic resistance, early intervention, and evidence standards for cancer programs.
Links MRD timing, antigen selection, vaccine manufacture, immune response, and recurrence endpoints into a recurrence-prevention decision gate.
Next-Generation Immuno-Oncology PlatformsSeparates IO platform promise from therapeutic-index reality across potency, specificity, resistance, safety, and combination logic.
Immune state, inflammatory memory, tolerance, autoimmunity, fibrosis, tissue resolution, neuro-immune control, and durable immune intervention endpoints.
Distinguishes remission achieved from durability solved by mapping persistence, sanctuary, and immune reconstitution risks.
Fibrosis as Failed ResolutionIdentifies the rate-limiting resolution node and the matched research move across persistence, scar integrity, and reversal measurement.
Immune Aging Supply ChainRoutes immune-aging programs to the binding supply-chain node before treating broad immune decline as one therapeutic target.
Therapeutic platforms that edit, replace, silence, repair, regulate, or compensate for DNA, RNA, chromatin, and variant-to-function disease mechanisms.
Classifies whether mitotic dilution, active erasure, or reactivation pressure will dominate before buyers commit to delivery, indication, or permanence strategy.
In Vivo Gene EditingTurns in-vivo editing from a modality story into a coupled-system failure-mode map.
RNA Editing & the Permanence SpectrumPositions RNA editing on a permanence spectrum so buyers do not confuse reversibility with durability or safety by default.
Cardiomyopathy, heart failure, arrhythmia, vascular biology, cardiometabolic risk, cardiac devices, genetic disease, and measurable cardiovascular outcome gates.
Resistance, pathogen threat ranking, fungal disease, host vulnerability, diagnostics, antimicrobial precision, surveillance gaps, and countermeasure design.
Maps fungal threat expansion against diagnostic timing, drug scarcity, resistance, toxicity, and host-risk stratification.
Precision AMR CountermeasuresUses mutational supply, diagnostic timing, pathogen burden, and combination logic to assess durability against resistance escape.
Small-population development, monogenic and mitochondrial disease, natural history, surrogate endpoints, variant interpretation, N-of-1 therapies, and evidence flexibility.
Routes variant interpretation toward rescue experiments instead of stopping at association, prediction, or annotation confidence.
Mitochondrial Medicine Permanence LadderMaps mitochondrial interventions onto a permanence ladder so buyers do not overbuild or underbuild the required correction.
Clinical AI, digital biomarkers, computational biology, prospective validation, deployment drift, sensor-derived measures, and decision utility.
Separates static generation wins from the harder validation problem: whether AI can predict dynamic biological response under prospective tests.
AI Clinical Validation & Digital BiomarkersTurns AI and digital biomarkers into validation-gate questions: prospective utility, generalization, drift, fairness, and endpoint acceptance.
Brain states, neural circuits, neurodegenerative biology, neural interfaces, closed-loop modulation, memory science, and neuro-immune control systems.
Diagnoses whether BCI/BSI decline is recoverable code drift or irreversible source loss before buyers overspend on the wrong layer.
Bioelectronic Neuro-Immune Closed LoopScores indication readiness by biomarker validity, sensing fidelity, decoding generalizability, circuit match, and substitution economics.
Engineering Memory / EngramsResolves the Lost-vs-Locked diagnostic gate before choosing re-access, editing, stabilization, reconstruction, or avoidance.
Neurodegeneration ConvergenceUses convergent detection to subtype disease, while requiring sign-labile biology and therapeutic-window logic before treatment spend.
New approach methodologies, organ-on-chip systems, biofabrication, perfusable tissues, xenotransplantation, platform devices, and translational engineering gates.
Routes a proposed context of use to its binding qualification gate before buyers spend on biological completeness.
Ovarian Aging Multi-ClockSeparates endocrine, follicular, mitochondrial, stromal, and functional clocks before buyers infer benefit from measurement movement.
Partial Epigenetic ReprogrammingMaps the rejuvenation-transformation margin so buyers can distinguish clock movement from functional, controlled, and safe benefit.
Perfusable Vascular NetworksEvaluates whether vascular networks are merely visible, truly perfusable, functionally mature, and integration-ready.
Xenotransplantation Durability CeilingMaps the durability ceiling across host tolerance, organ-specific failure physiology, immune compatibility, and organ-scale function.
Domain pages are field-first maps: what changed recently, what is measurable, what remains unresolved, and which Zemi Dossiers fit the active decision gates.
A Zemi Dossier is the output of a process no individual reader can replicate: hundreds of sources synthesized, every claim independently audited, and every number traceable to where it came from — compressing months of analyst work into one decision-ready package.
See how it's builtHundreds of papers, trials, registries, regulatory records, and company signals are read and reconciled — surfacing cross-field connections no single analyst spans.
An AI auditor resolves each citation against live databases and tests whether the source actually supports the claim, so issues are corrected before release.
Claims carry verbatim excerpts and page anchors; figures and power rows map back to identifiers. You can audit the dossier instead of trusting it.
What would take a team months to assemble — less thoroughly — arrives decision-ready, with the excluded and quarantined work preserved.
Nine medical domains, each with field-first decision dossiers — every package pairs a research report with an Evidence & Decision Workbook and power-calculated next studies.